6 Understanding the EEG
An electroencephalogram (EEG) is a test that records the brain’s electrical activity. It is the single most important test for diagnosing and managing epilepsy, and for most families it is one of the first tests their child will have after a seizure.
The good news is that an EEG is completely painless and non-invasive. Nothing goes into the body, and no electricity is sent into the brain. The electrodes on the scalp simply listen to the brain’s own natural signals and record them.
6.1 Why Is an EEG Done?
Seizures are caused by abnormal bursts of electrical activity in the brain. Between seizures, and sometimes even during them, the EEG can pick up patterns that help confirm a diagnosis, identify the seizure type, and pinpoint where in the brain the activity is coming from. Your child’s neurologist may order an EEG to look for signs of epilepsy even if no seizure was captured during the recording because certain abnormal patterns show up between seizures as well.
Beyond diagnosis, EEG is used to monitor how well treatment is working, to help classify the epilepsy syndrome, and to guide decisions about whether and when medications might eventually be reduced or stopped.
6.2 Types of EEG
Not all EEGs are the same. The type your child’s doctor orders depends on what question needs to be answered.
A routine EEG is the most common type and usually takes 20 to 40 minutes. It is done in a clinic or hospital with electrodes placed on the scalp, and it captures a brief snapshot of the brain’s electrical activity. It is often the first EEG a child will have.
A sleep-deprived EEG asks your child to sleep less than usual the night before the test. Sleep deprivation makes certain epilepsy patterns more visible, and recording during drowsiness or light sleep significantly increases the chance of capturing abnormal activity. Your care team will give you specific instructions about how much sleep to skip.
An ambulatory EEG is a portable version that your child wears at home for 24 to 72 hours or longer. The electrodes stay attached, and a small recording device is worn on a belt or in a pouch. Your child can go about most normal activities during the recording. This type is useful when events are frequent enough that they are likely to be captured over a longer period, or when routine EEG has not given a clear answer.
Video-EEG monitoring is the most comprehensive option and is done during a hospital stay, usually lasting several days. Continuous EEG recording is combined with video cameras so that the clinical appearance of a seizure and its electrical signature can be seen simultaneously. This is the gold standard for determining exactly where seizures start in the brain and is a key part of any presurgical evaluation.
6.3 What to Expect During a Routine EEG
6.3.1 Getting ready
On the day of the EEG, your child’s hair should be clean and completely dry, without any conditioner, gel, or styling products as these interfere with the electrode contact. Regular medications should be taken as usual unless your doctor specifically instructs otherwise.
For younger children, it helps to explain what will happen beforehand in simple terms: a technician will put small stickers on their head, it will not hurt, and they get to lie still and relax. Bringing a favourite comfort item is encouraged.
6.3.2 Electrode placement
When you arrive, a technician will measure your child’s head and mark the correct positions for the electrodes using a soft pencil. Each spot is gently cleaned, and small metal disc electrodes are attached using a gel or paste that helps conduct the signal. The electrodes are placed in standardized positions that cover all regions of the brain. The placement process takes about 15 to 20 minutes and is the part that children sometimes find tedious, though it is not painful.

6.3.3 The recording
Once the electrodes are in place, your child will sit in a comfortable chair or lie on a bed for 20 to 40 minutes while the recording takes place. Staying relaxed and still is important, as muscle movement creates electrical noise that can obscure the brain signals. The technician will ask your child to open and close their eyes at various points and will watch the brain activity on a screen in real time.
During the recording, two brief activation procedures are routinely used. The first is hyperventilation, in which your child is asked to breathe deeply and rapidly for three to five minutes. This lowers the carbon dioxide level in the blood and can bring out certain epilepsy patterns, particularly those associated with absence epilepsy. It may cause mild lightheadedness or tingling, which is normal and passes quickly. The second is photic stimulation, in which a strobe light flashes at different frequencies. This tests for photosensitivity, which is a feature of a small number of epilepsy syndromes. If your child finds the flashing uncomfortable, they can close their eyes.
Most EEGs do not capture an actual seizure, and that is completely fine. The test is still valuable because it can show abnormal patterns between seizures, called interictal discharges, that strongly support a diagnosis of epilepsy. A normal EEG during a brief recording does not rule out epilepsy.
6.3.4 After the test
Electrode removal takes only a few minutes. The paste or gel washes out with shampoo, though it may take two or three washes to remove completely. Your child can resume all normal activities immediately. If the EEG involved sleep deprivation, they should not drive home.
6.4 Reading the EEG: What the Patterns Mean
An EEG is useful in two distinct ways. The first is to directly catch a seizure, to record the electrical event itself and study it. This tells us whether an episode is truly a seizure, what type it is, and where in the brain it is coming from. The second is to study the brain’s background activity, the electrical landscape between seizures. Even without capturing a seizure, this background recording can reveal important clues.
Think of it this way: if a seizure is a fire, then the abnormal patterns seen between seizures are like sparks. The sparks are not the fire itself, but they tell us something important, namely that this brain has a tendency to generate them, and where. A neurologist reading an EEG is looking for both: evidence of fire, and evidence of sparks.
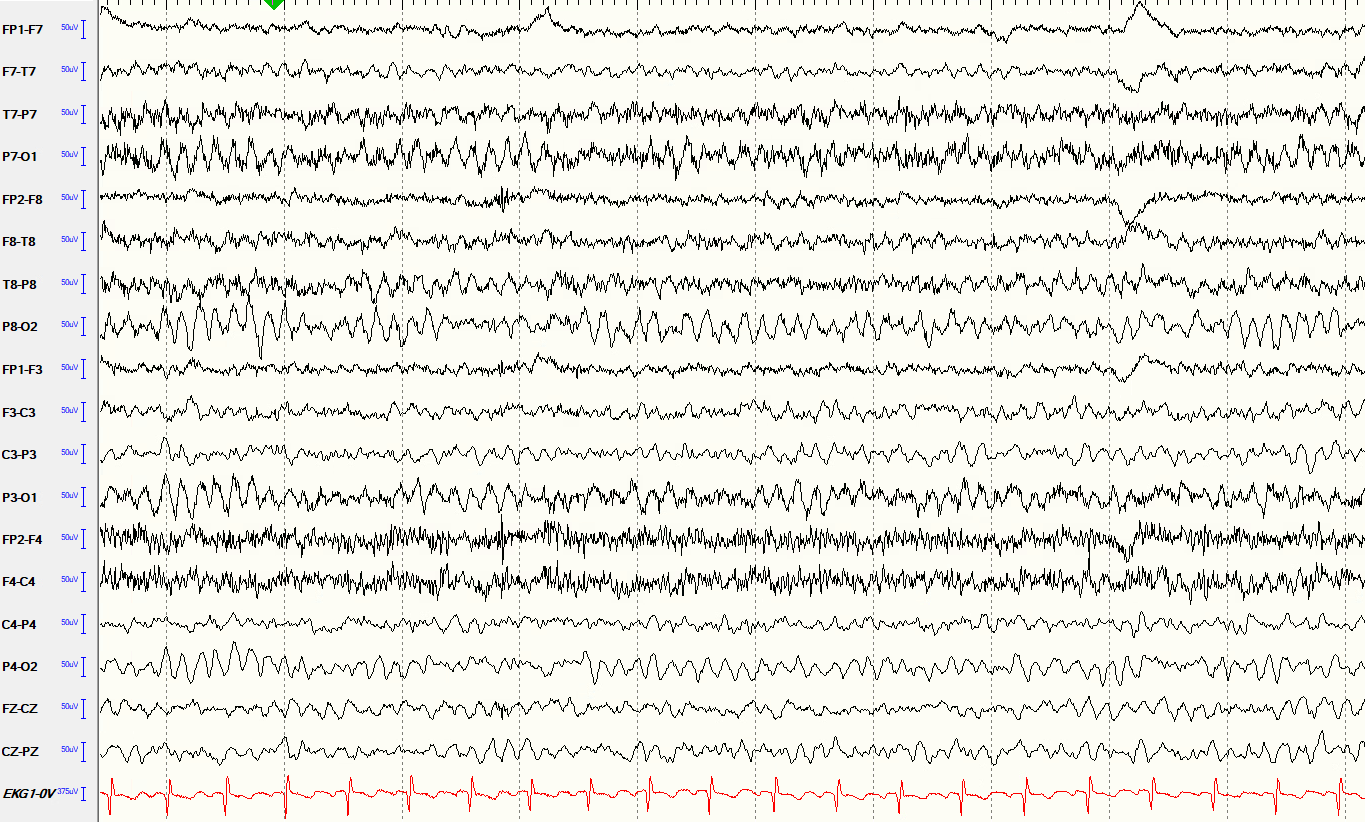
6.4.1 The normal EEG
A normal EEG shows organized, rhythmic electrical activity that changes predictably with age, alertness, and eye opening and closing. In a relaxed, awake child with eyes closed, the dominant pattern is a smooth, regular wave called the alpha rhythm, seen most prominently over the back of the head. As a child becomes drowsy or falls asleep, the pattern shifts in characteristic ways that the neurologist can recognize. A normal EEG provides important reassurance but does not by itself rule out epilepsy, because abnormal discharges are intermittent and may not occur during the recording window.
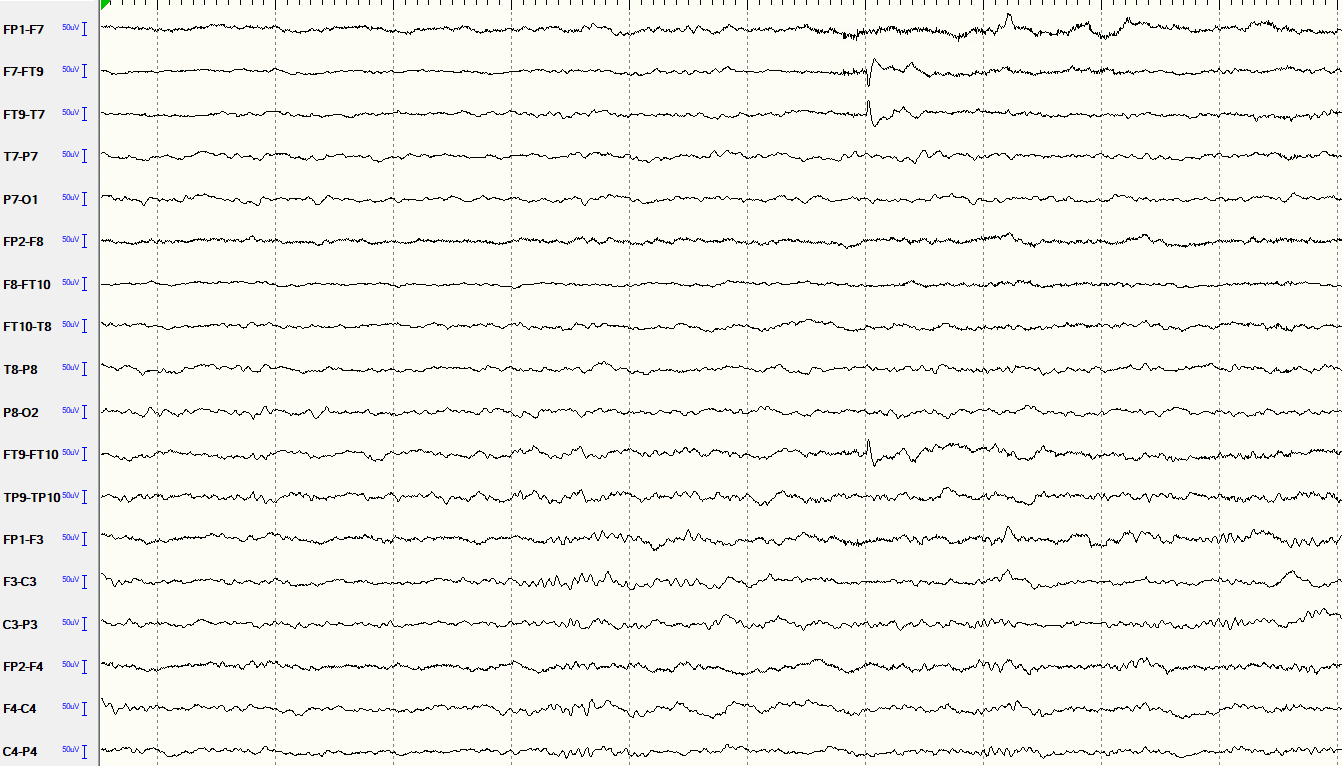
6.4.2 Interictal discharges
Between seizures, some children with epilepsy show brief abnormal electrical events called interictal discharges: spikes, sharp waves, or spike-and-wave complexes that stand out sharply against the normal background. These are the “sparks.” They are not seizures themselves, but they tell us that the brain has an underlying tendency toward abnormal electrical firing. Their shape, location, and distribution provide important clues about the type of epilepsy. For example, generalized spike-and-wave discharges at three cycles per second are characteristic of absence epilepsy, while focal spikes over the central and temporal regions are typical of self-limited epilepsy with centrotemporal spikes (BECTS).
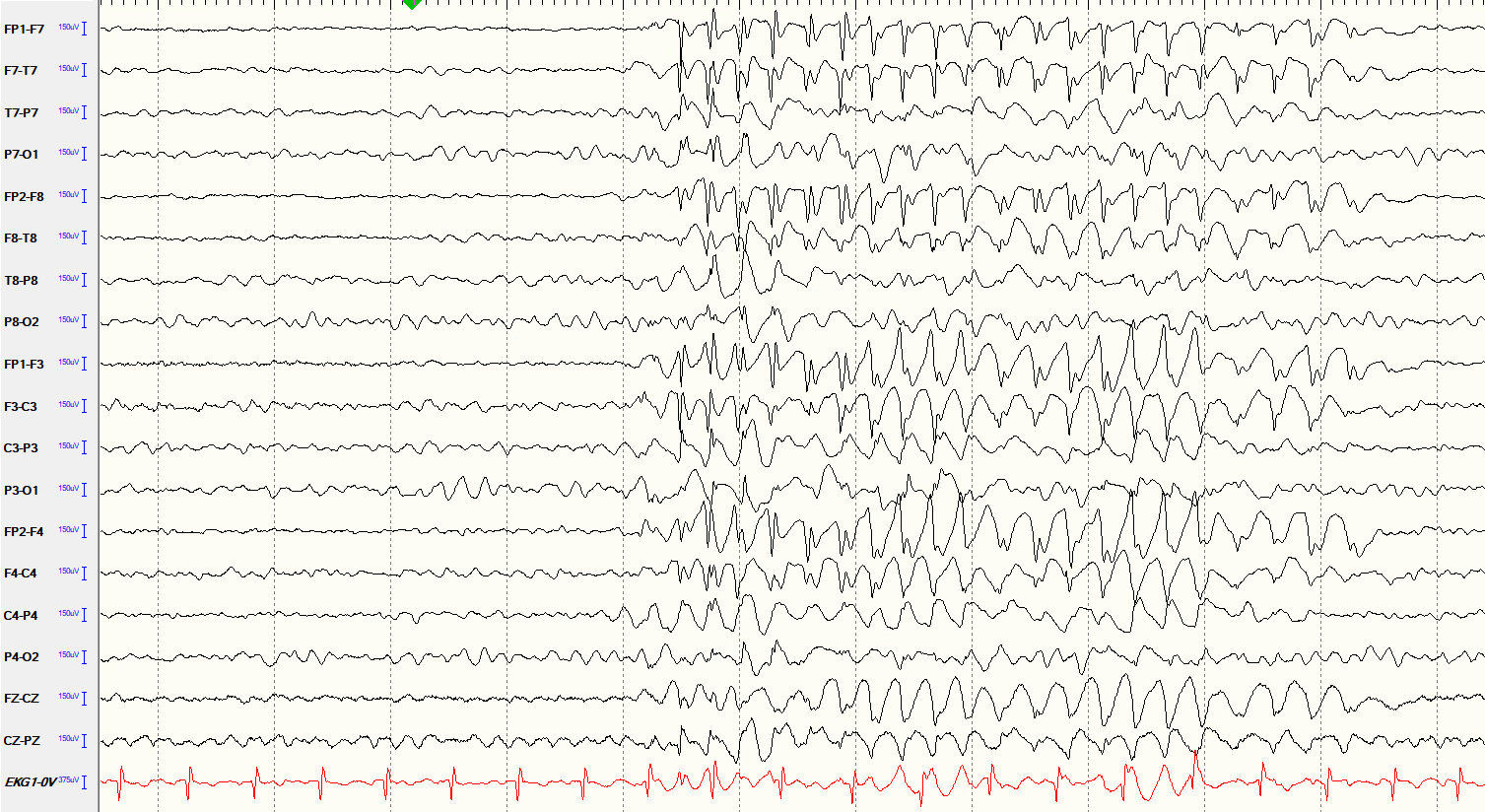
6.4.3 Seizure activity
When a seizure is recorded, the EEG shows a dramatic change from the background, typically a sudden buildup of rhythmic, repetitive activity that evolves in frequency and amplitude over the course of the event, then gradually resolves. The appearance varies depending on the seizure type and where it starts. Seeing a seizure on EEG simultaneously with video of the clinical event is the most powerful way to confirm the diagnosis and characterize the epilepsy. This is the primary goal of inpatient video-EEG monitoring.
6.5 A Few Important Points About EEG Results
A normal EEG does not rule out epilepsy. About half of all people with epilepsy have a normal first EEG. Epileptic discharges are intermittent: they may simply not occur during the brief recording window. If the clinical suspicion for epilepsy remains high, a repeat EEG, a sleep-deprived EEG, or a longer ambulatory recording may be recommended.
An abnormal EEG does not automatically mean epilepsy. A small number of people without epilepsy show epileptiform-looking patterns on EEG. The result must always be interpreted in the context of the clinical history, the examination, and other test findings. Your child’s neurologist will put all of this together before reaching a conclusion.
The EEG is one piece of a larger picture but always interpreted alongside everything else known about your child.