8 Other Types of Imaging
For most children with epilepsy, a high-quality MRI may be the only imaging test needed. But for some children, especially those whose seizures are not controlled by medication, or whose MRI did not find a clear cause, there are additional tests that can give important information about how different parts of the brain are working.
These tests are not routinely done at every hospital. They are typically offered at specialized epilepsy centres as part of a presurgical evaluation, and they are almost always reviewed together as a group rather than used alone. No single test gives the full picture; each one adds a different piece of information.
8.1 PET Scan
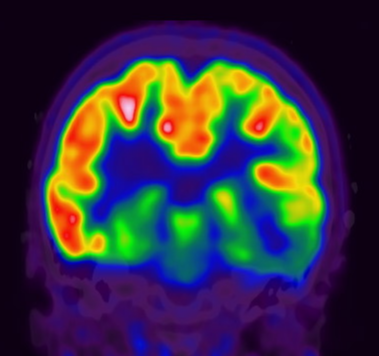
A PET scan, short for positron emission tomography, measures how active different parts of the brain are by tracking how they use energy. Brain cells need glucose (a type of sugar) to function. Before the scan, a small amount of a mildly radioactive glucose tracer is injected into a vein. The scanner then detects where in the brain that tracer is being used.
In epilepsy, PET is almost always done between seizures, when the brain is in its resting state. The area of the brain responsible for seizures often uses less energy than the surrounding tissue during this resting period, so it shows up as a dimmer, cooler region on the scan. Even when the MRI looks completely normal, a PET scan can sometimes point to the part of the brain where seizures are coming from.
The scan itself is painless. After the tracer injection, your child will rest quietly in a low-stimulation room for about 30 to 60 minutes while the tracer travels to the brain. The scanning portion then takes roughly 20 to 30 minutes lying still inside the machine, which looks similar to a CT scanner: a wide, open ring rather than the narrow tunnel of an MRI. The radiation dose is low, similar to other nuclear medicine tests like a bone scan.
8.2 SPECT Scan
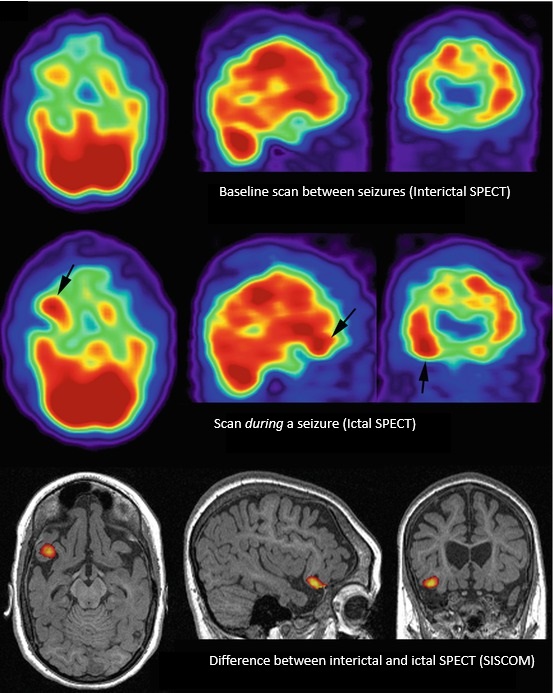
A SPECT scan, short for single photon emission computed tomography, measures blood flow in the brain. During a seizure, the parts of the brain involved receive a sudden rush of blood. A SPECT scan done during a seizure can capture that rush and pinpoint exactly where it happened.
This is called an ictal SPECT, and it is the most valuable version of the test. It requires careful preparation: a radioactive tracer must be injected within seconds of a seizure beginning, while the seizure is still happening. For this reason, it is only done during an inpatient stay in an epilepsy monitoring unit, where nurses are trained and ready to inject the tracer the moment a seizure starts. The scan is done after the seizure has ended, since the tracer stays fixed in the brain tissue for long enough to image it.
The results are then compared to a scan done between seizures (called an interictal SPECT) to identify which area showed the biggest increase in blood flow. The difference between the two scans, often displayed as a colour map overlaid on the MRI, highlights the seizure origin zone.
Like the PET scan, SPECT involves a low dose of radiation and the scanning itself is painless.
8.3 fMRI
Functional MRI uses the same scanner as a standard brain MRI, but instead of just taking a picture of brain structure, it detects which areas of the brain become active in response to specific tasks. When a brain region is working, it receives more oxygenated blood, and fMRI is sensitive enough to detect that change.
In epilepsy, fMRI is used to map critical brain functions before surgery. While lying inside the scanner, your child will be asked to do simple tasks, such as tapping their fingers, looking at pictures, or answering questions, and the scan identifies which parts of the brain respond. The most important areas to map are usually language (both the ability to speak and the ability to understand) and movement.
The goal is to make sure the surgical team knows exactly where these functions are located before removing any tissue. This is especially important because these areas can be in slightly different locations from one person to the next, and the locations can shift in children who have had early brain injury or seizures.
fMRI involves no injections and no radiation. It does require the same degree of cooperation as a standard MRI, meaning lying still in the scanner for 45 to 60 minutes, and some younger children may need sedation, though sedation limits how well the tasks can be performed.
8.4 Magnetoencephalography
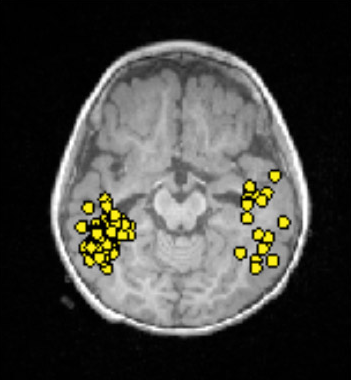
Magnetoencephalography (MEG) is a test that measures the tiny magnetic fields produced by electrical activity in the brain. Every time a group of neurons fires, it creates a small magnetic pulse. MEG detectors are sensitive enough to pick up these pulses from outside the skull.
In some ways MEG is similar to an EEG, which measures the same electrical activity using electrodes on the scalp. The difference is that magnetic fields travel through the skull and scalp without being distorted, whereas electrical signals are blurred by the time they reach the scalp electrodes. This means MEG can often pinpoint the source of abnormal brain activity more precisely than a standard EEG.
During the test, your child sits or reclines with their head positioned inside a large helmet-shaped device lined with several hundred sensors. The test is completely non-invasive: there are no needles, no injections, and no radiation. The recording typically takes one to two hours. Because the sensors need to detect extremely faint magnetic fields, the room is specially shielded from outside interference, and your child will need to stay reasonably still.
MEG is only available at a small number of specialized centres. When it is available, it is most useful in children with a normal or unclear MRI, or when other tests have not agreed on where the seizures are coming from.
8.5 How These Tests Work Together
Each of these tests answers a slightly different question:
- MRI shows what the brain looks like
- PET shows where the brain is less active between seizures
- SPECT shows where the brain is most active during a seizure
- fMRI shows where critical functions like speech and movement are located
- MEG shows where abnormal electrical activity is coming from
No single test is enough on its own. The epilepsy team reviews all of the results together, alongside EEG recordings, neuropsychological testing, and the clinical history, before making any recommendation about surgery. The goal is for multiple tests to point to the same area, which increases confidence that removing or disconnecting that area is both safe and likely to help.