9 Genetic Testing
When a child is diagnosed with epilepsy, one of the first questions families ask is: why did this happen?
For many children, the answer may be explained by their genes. Genes are the instructions that guide how our bodies develop and function. When one of those instructions contains a small error, it can affect how the brain’s electrical system works, making seizures more likely. Over the past two decades, researchers have identified more than 200 genes that can cause or contribute to epilepsy, and new ones are discovered every year.
Genetic testing is a way of searching for those errors. It is not a single test, but rather a family of different tests, each looking at genes in a different way. Not every child with epilepsy needs genetic testing, and not every test will find an answer. However, for the right child at the right time, it can be one of the most important pieces of the diagnostic puzzle.
9.1 Genetics 101
To understand what genetic testing is looking for, it helps to have a mental picture of how genetic information is organized in the body.
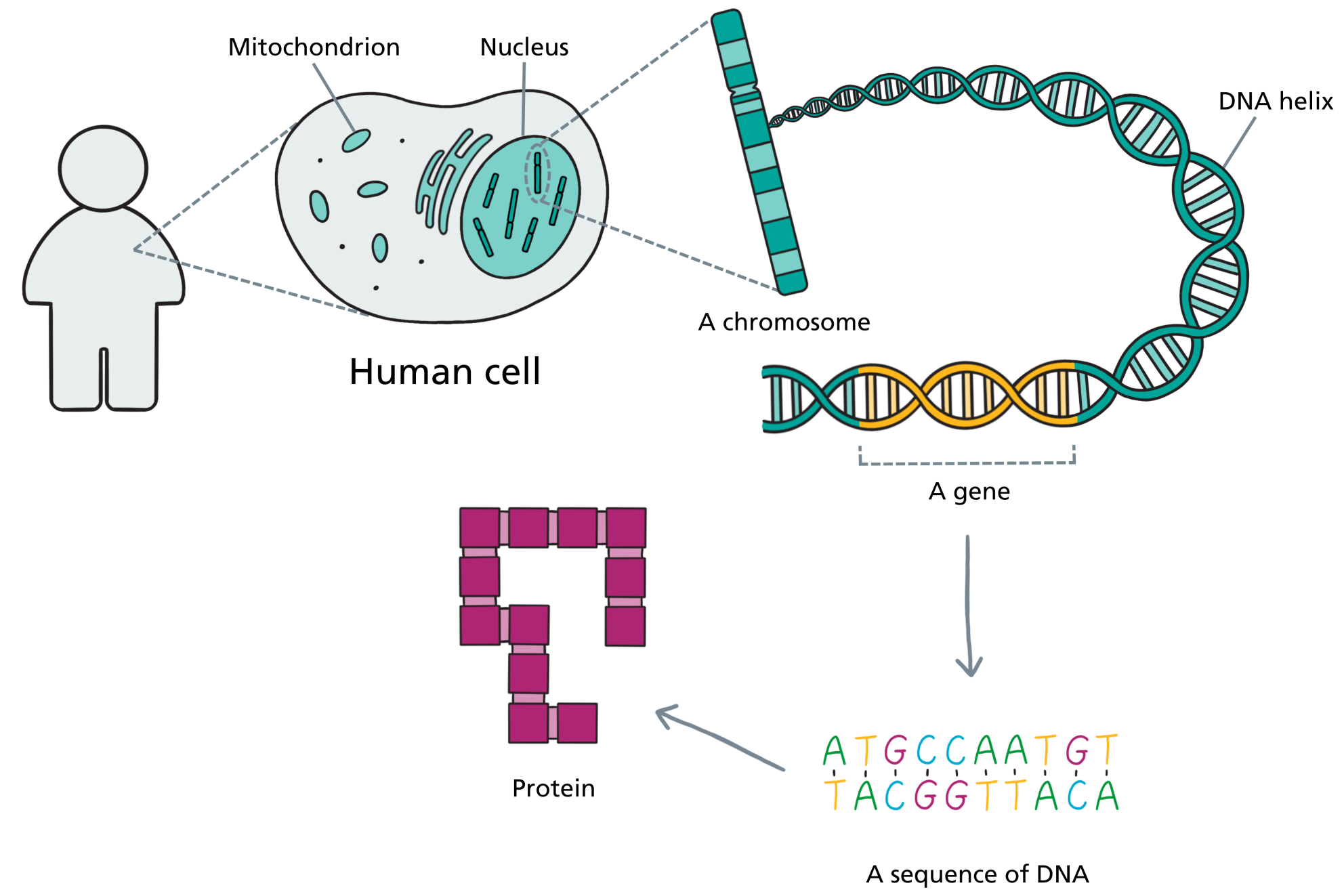
Every cell in your child’s body contains a nucleus, and inside that nucleus is the complete set of genetic instructions for building and running a human being. Those instructions are packaged into structures called chromosomes. Zoom in further and each chromosome is made of a long, tightly coiled molecule of DNA. Zoom in further still and you reach the level of individual genes: specific stretches of DNA that each carry the instructions for making a particular protein. And at the finest level of all, those instructions are written in a sequence of four chemical letters, A, T, G, and C, strung together in a precise order.
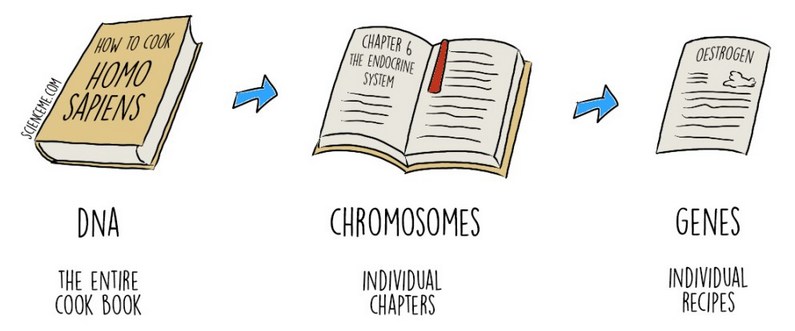
A helpful way to think about all of this is through the analogy of a book. Your child’s entire genetic blueprint, the genome, is like a vast instruction book for building and running a human being. It contains everything the body needs to know: how to grow a brain, how to wire its connections, how to keep the heart beating, how to heal a cut. It is the most complex instruction manual ever written, and every cell carries a complete copy.
The genome is organized into chromosomes, which are like the chapters of that book. Humans have 46 chromosomes in total, arranged in 23 pairs: one set inherited from each parent. Within each chromosome, the instructions are broken down further into genes, which are like individual recipes within a chapter. Each gene carries the instructions for making a specific protein, and those proteins do the actual work of the body: building structures, carrying signals, controlling chemical reactions. The brain alone relies on thousands of different proteins working in precise coordination, including the ion channels and receptors that regulate electrical activity in neurons.
The “words” in each recipe are written in DNA using those four chemical letters. A typical gene might be thousands of letters long. When those letters are in the right order, the recipe works correctly. When there is a spelling error, even a single wrong letter, the protein it produces may not work as it should.
In epilepsy, genetic testing is essentially proofreading. Depending on the test, it may scan for entire missing or duplicated chapters (chromosomal microarray), check the spelling in a curated list of known recipes (gene panel), read every recipe in the book from cover to cover (whole exome sequencing), or read the entire book including all the footnotes and annotations between recipes (whole genome sequencing). Each approach has different strengths, and the right choice depends on what the clinical team is looking for.
If you would like to explore these concepts further, the U.S. National Library of Medicine hosts a free, patient-oriented guide called Understanding Genetics that covers cells, DNA, genes, inheritance patterns, and the types of genetic disease in accessible language.
9.2 Who Needs Genetic Testing?
Genetic testing is not routinely recommended for every child with epilepsy. For a child whose seizures started after a clear cause, for example a birth injury, a stroke, a brain infection, genetics is less likely to provide additional useful information. But in many other situations, it may be well worth considering.
Children who are most likely to benefit include those whose seizures began in infancy or early childhood, particularly if no structural cause has been found on MRI. Genetic testing is especially helpful when epilepsy comes alongside developmental delay, intellectual disability, autism, or other neurological features; combinations that suggest the brain may have been wired differently from early on. Children with a type of epilepsy that does not fit neatly into a recognized pattern, those whose seizures have not responded to multiple medications, and those with a family history of epilepsy are also good candidates. Certain specific epilepsy syndromes (e.g. Dravet syndrome, infantile spasms, Lennox-Gastaut syndrome) carry a high enough chance of having a genetic cause that testing is now considered a standard part of their evaluation.
It is worth knowing that finding a genetic cause does not always mean the epilepsy was “inherited” in the traditional sense. Many genetic changes in children with epilepsy arise anew: what geneticists call de novo mutations, meaning neither parent carries the same change, and it was not passed down through the family. This is an important distinction, and it is one of the things a genetic counsellor can help clarify.
If you are unsure whether genetic testing is right for your child, the best starting point is a conversation with your child’s epileptologist or neurologist. They can review your child’s specific history and help decide which tests, if any, make the most sense.
9.3 Types of Genetic Tests
Choosing a genetic test requires weighing several factors: how broad the search needs to be, how urgently a result is needed, what other information might come with the answer, and what the laboratory can realistically detect. The following tests are the ones most commonly used in epilepsy care today, roughly in order from most targeted to most comprehensive.
Chromosomal Microarray
The chromosomal microarray (sometimes called a CMA or chromosome array) does not look inside individual genes. Instead, it scans across all the chromosomes at once, searching for segments of genetic material that are missing or duplicated. These extra or absent chunks of DNA are called copy number variants, or CNVs. Some CNVs disrupt genes that are important for brain development, leading to epilepsy alongside other neurological features.
Chromosomal microarray is abnormal in roughly 5 to 10% of children with epilepsy, and the yield is higher in children who also have developmental delay, intellectual disability, or autism. It is often one of the first genetic tests ordered, partly because it has been available for longer than other methods and partly because it is reasonably priced and widely accessible.
Epilepsy Gene Panels
Gene panels use a technology called next-generation sequencing to look inside many genes at once: typically somewhere between 100 and 500 genes known to be associated with epilepsy. Rather than scanning for large missing or duplicated chunks, panels read the detailed sequence of each gene’s instructions, looking for small errors in the genetic “spelling” that could disrupt how the gene works.
The appeal of gene panels is that they are focused and relatively fast. The tradeoff is that they can only find what they are looking for: if the cause of a child’s epilepsy turns out to be a recently discovered gene not yet included on the panel, it will be missed. Panels find a definitive cause in approximately 20% of children tested.
Whole Exome Sequencing
The exome is the portion of the genome that contains all of the protein-coding genes, roughly 20,000 genes in total. Whole exome sequencing, or WES, reads the detailed sequence of all of them at once. This makes it far broader than a gene panel, and better positioned to catch causes that were not suspected in advance or that involve genes too recently discovered to be on commercial panels.
Exome sequencing is often done as a “trio,” meaning the child and both parents are tested at the same time. This approach makes it much easier to determine whether a genetic change is new (de novo) or was inherited, and it helps filter out the many genetic variants that are simply normal human variation rather than disease-causing.
Because exome sequencing looks at so many genes, results can take several weeks to several months to return, and interpretation is more complex. It establishes a definitive diagnosis in approximately 24 to 30% of children with previously unexplained epilepsy. Importantly, exome data can be reanalyzed over time. If no cause is found today, the same data can be revisited in a few years as new epilepsy genes are discovered.
Whole Genome Sequencing
Whole genome sequencing goes one step further than exome sequencing, reading not just the protein-coding regions but essentially the entire genetic blueprint, including the large stretches of DNA between genes that regulate how and when those genes are switched on and off. This makes it the most comprehensive test currently available.
Genome sequencing has the highest diagnostic yield of any genetic test in epilepsy, identifying a cause in nearly half of children who undergo it in the right clinical setting. It is also the most complex test to interpret, and it is not yet universally available as a routine clinical test. At most centres it is reserved for children in whom other testing has not found an answer, though guidelines are increasingly recommending it, or exome sequencing, as a first-tier test for children with unexplained epilepsy.
9.4 Why Does the Test Matter for Treatment?
Finding the genetic cause of epilepsy is not just about having an answer. For some conditions, it directly changes treatment. Children with Dravet syndrome (usually caused by a change in the SCN1A gene) need to avoid certain anti-seizure medications that can make their seizures worse. Children with a rare condition called pyridoxine-dependent epilepsy respond to high doses of vitamin B6 rather than standard medications. Several newer treatments (and many ongoing clinical trials) are targeted specifically at children with particular genetic diagnoses. The right test, at the right time, can genuinely change the path of care.
9.5 How Is the Sample Collected?
Most genetic testing for epilepsy requires only a blood draw. Some laboratories can also analyze a saliva sample instead, which may be easier for young children or those with difficult venous access. The sample is sent to a specialized genetics laboratory, where DNA is extracted and analyzed. Results typically take anywhere from two weeks to several months depending on the type of test.
9.6 Understanding the Results
Receiving the results of genetic testing can feel like a significant moment, and the range of possible outcomes is wider than many families expect. Results generally fall into three categories.
A positive result, also called a pathogenic or likely pathogenic variant, means the laboratory has found a genetic change that is known or very likely to be the cause of your child’s epilepsy. This is the result families hope for, because it provides a clear explanation and can guide treatment decisions, give the clinical team a better sense of prognosis, and open doors to condition-specific support communities and clinical research. It also has implications for other family members, including the possibility of carrier testing or reproductive planning, which is one of the important reasons to involve a genetic counsellor.
A negative result means the test did not find a genetic change that explains your child’s epilepsy. It is important to understand that a negative result does not prove that genetics played no role. It means only that the current test did not detect a cause within its scope. Our knowledge of epilepsy genetics is still growing rapidly, and a test that comes back negative today may yield an answer when reanalyzed in two or three years as the field advances. For this reason, many epilepsy genetics teams build in a plan for periodic reanalysis of stored data.
A variant of uncertain significance (VUS) is perhaps the most challenging result to receive. It means the laboratory found a genetic change that looks unusual, but there is not yet enough evidence to say with confidence whether it is the cause of the epilepsy or simply a benign variation in that individual’s genome. A VUS is not a diagnosis, and it should not be treated as one. Over time as more children with similar variants are identified and studied, a VUS may eventually be reclassified as either pathogenic or benign. Your child’s geneticist or epileptologist will monitor this and notify you if the classification changes.
9.7 Implications Beyond Epilepsy
Genetic testing carries implications that go well beyond a laboratory report. Results can affect how family members understand their own health, influence decisions about future pregnancies, and sometimes raise complicated questions about insurance. For these reasons, it is strongly recommended that families have thorough counselling, both before testing to understand what to expect, and after testing to make sense of the results and their implications.
This counselling may be provided by your child’s epileptologist, a neurologist with expertise in epilepsy genetics, or a genetic counsellor, depending on the centre and the complexity of the results. What matters is that someone on your team takes the time to walk through what the testing is looking for, what each possible result would mean, how long it will take, and what the plan is if no clear answer is found.
Informed families are better prepared for whatever the results bring, including the uncertainty that is sometimes the only answer genetics can offer, at least for now.