7 Brain Imaging
When a child has seizures, one of the first questions your doctor may ask is whether there is something visible in the brain that might be causing them. Brain imaging answers this question by creating detailed pictures of the brain’s structure. The results can reveal scarring, abnormal tissue development, tumors, or vascular malformations that help explain why seizures are happening and guide decisions about treatment.
This chapter covers the two main types of brain imaging used in epilepsy, MRI and CT, and explains what to expect during each test and how to make sense of the results. For children being evaluated for epilepsy surgery, additional specialized imaging tests are available; these are covered separately in the chapter on Advanced Brain Imaging.
7.1 Is Imaging Always Necessary?
Not every child who has a seizure needs a brain MRI, and not every child with epilepsy does either. The decision to image depends on the full clinical picture, including the type of seizures, the examination findings, and the EEG results.
For some children, brain imaging can be safely deferred or is not required at all:
Classic epilepsy syndromes. Several well-recognized childhood epilepsy syndromes are defined by their clinical and EEG features alone, and are not associated with structural brain abnormalities. In these cases, MRI typically does not change the diagnosis or treatment. Syndromes in this category include childhood absence epilepsy, juvenile absence epilepsy, juvenile myoclonic epilepsy (JME), and self-limited epilepsy with centrotemporal spikes (BECTS/SELF-CTS).1
A first unprovoked seizure with no concerning features. In a child with a single seizure, no focal features on history or examination, and no focal abnormalities on EEG, routine neuroimaging is generally not recommended. Studies suggest that while brain abnormalities appear on imaging in up to a third of children after a first seizure, only about 2% show findings that would immediately change management, and these are almost always in children with focal seizures or other clinical red flags.2
Seizures with a clear provoking cause. When a seizure is clearly triggered by a reversible cause, such as a metabolic disturbance, electrolyte abnormality, fever, or acute illness, imaging may be deferred if there are no focal neurological findings.3
In all cases, the decision is individualized. Your child’s neurologist will weigh the clinical context carefully before deciding whether and when to image.
7.2 MRI: The Cornerstone of Epilepsy Imaging
When imaging is indicated, magnetic resonance imaging (MRI) is the test of choice. It uses powerful magnets and radio waves to build detailed, cross-sectional pictures of brain tissue. There is no radiation involved, and the images can be acquired in many different ways to highlight different features of the brain’s structure.
7.2.1 What an MRI looks like
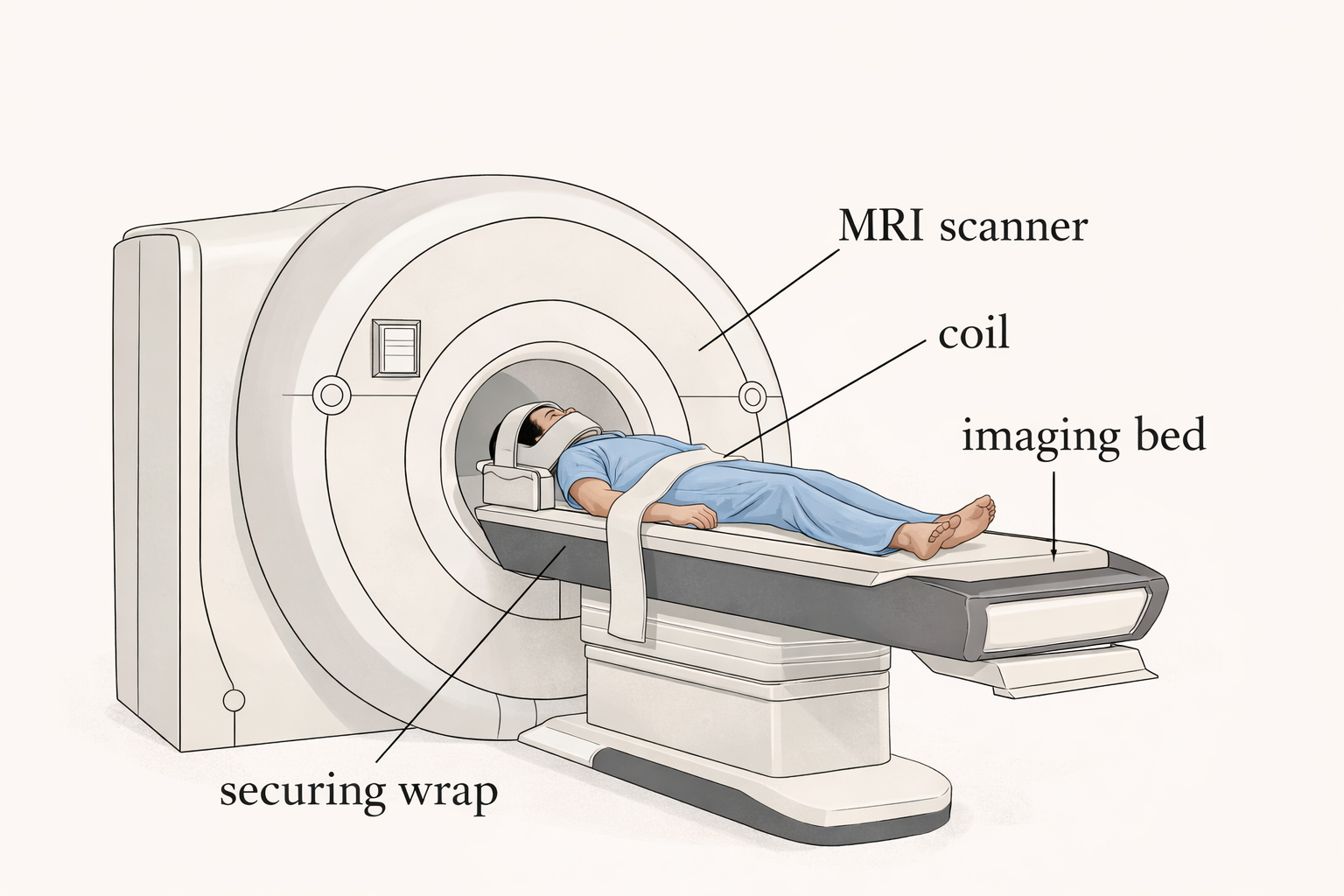
For most families, the MRI machine itself is the first surprise. It is a large, cylindrical scanner, shaped like a donut, with a sliding table that moves the patient into the opening at its centre. The machine is loud during the scan, producing a series of knocking and buzzing sounds as the magnetic fields shift. Children are given earplugs or headphones, and many centres offer music or audiobooks to help pass the time.
The scan typically takes 45 to 75 minutes, depending on how many imaging sequences are needed. The most important requirement is staying as still as possible, because movement blurs the images and can make subtle findings harder to detect. For younger children or those who have difficulty staying still, sedation or general anesthesia is often used to ensure a high-quality result.
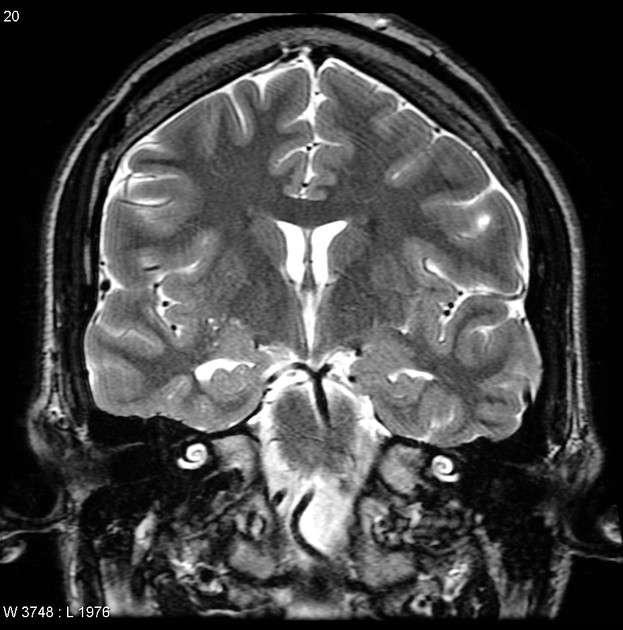
7.2.2 What an epilepsy MRI looks for
Not all MRI scans are the same. A standard brain MRI, the kind ordered for headaches or dizziness at a general hospital, is designed to detect obvious abnormalities like tumors or strokes. An epilepsy protocol MRI is designed specifically to look for the kinds of subtle changes that cause seizures. It uses thinner image slices, specialized sequences, and extra attention to the temporal lobes, which are involved in many seizure types. This makes it significantly more sensitive for findings that a routine MRI might miss entirely.
Some of the most important findings an epilepsy MRI looks for include:
- Hippocampal sclerosis: scarring in the hippocampus, a memory-related structure deep in the temporal lobe, and one of the most common causes of drug-resistant temporal lobe epilepsy
- Focal cortical dysplasia: a patch of abnormally developed cortex that can be very subtle, even on high-quality imaging
- Cortical tubers: seen in tuberous sclerosis complex
- Vascular malformations: such as cavernous malformations or arteriovenous malformations
- Evidence of prior injury: including stroke, hemorrhage, or hypoxic injury
In many children, however, the MRI comes back entirely normal. This is covered further below.
7.2.3 MRI field strength
MRI machines are measured in units called Tesla (T), reflecting the strength of the magnetic field. The most common hospital scanners are 1.5T machines. Higher-field 3T scanners offer better image resolution and are now preferred at most epilepsy centres, because they are more likely to detect subtle abnormalities, particularly small areas of cortical dysplasia that can be invisible on lower-field imaging.
Some specialized epilepsy research centres also have access to 7T MRI, which provides exceptional detail. These are not widely available and are typically used only in the most complex cases.
7.2.4 What to expect: a practical guide
Before the scan, there are no dietary restrictions and your child should take their regular medications. You will be asked to remove all metal from your child’s clothing and belongings, because the magnetic field is always active inside the scanner room and can attract metal objects with significant force. The team will ask about any metal implants, prior surgeries, pacemakers, or cochlear implants, all of which must be reviewed before proceeding.
During the scan, a staff member will position your child on the table, place a specialized head coil to improve image quality, and stay in communication via intercom throughout. The scan proceeds through a series of sequences, each with its own sound pattern.
After the scan, no recovery time is needed unless sedation was used. Your child can eat, drink, and resume normal activities immediately. Results are typically interpreted by a neurologist within a few days to a week.
If your child has ever had surgery involving metal plates, screws, or clips, or uses a device such as a cochlear implant or pacemaker, tell the MRI team well in advance. Some implants are MRI-compatible and some are not. The MRI department will review the specifics before scheduling.
7.3 CT Scanning: A Quicker Look When It’s Needed
A CT (computed tomography) scan uses X-rays to produce rapid images of the brain. While it provides far less structural detail than MRI for epilepsy purposes, there are situations where it is the right tool: in an emergency when speed matters, when MRI is not possible due to a non-compatible implant, or when the clinical question is about acute bleeding or injury rather than subtle structural changes.
For most children with epilepsy, the evaluation and ongoing imaging will rely on MRI. An early CT scan does not replace the need for a high-quality epilepsy-protocol MRI.
7.4 Understanding Your Child’s Imaging Results
7.4.1 When the MRI is normal
A normal MRI does not mean there is no epilepsy, and it does not mean the seizures are not real. Between 20 and 30 percent of people with epilepsy have a completely normal MRI. The underlying cause may involve changes at a microscopic level or it may involve a genetic or metabolic mechanism that does not produce any visible structural change at all.
When the MRI is normal, the diagnosis rests on the EEG findings, the seizure type, and the overall clinical picture. Medications work regardless of whether the MRI shows a cause, and a normal result does not change the general approach to treatment.
7.4.2 When something is found
A finding on MRI can mean very different things depending on the context. Some findings (e.g. hippocampal sclerosis in a child with temporal lobe epilepsy) point directly to the seizure source and may open the door to surgical evaluation. Others may be incidental: small cysts, minor vascular variants, or developmental changes that are entirely unrelated to the epilepsy and require no action.
Your neurologist will explain what any finding means for your child specifically. Not every abnormality seen on MRI is the cause of the seizures, and not every finding requires a change in treatment.
7.4.3 Imaging and surgery
For children whose seizures do not respond to medication, high-quality brain imaging becomes especially important. The goal of presurgical evaluation is to identify a clearly defined area of the brain responsible for the seizures that can be safely removed or disconnected. In addition to MRI, specialized tests such as PET, SPECT, fMRI, and MEG can each contribute different pieces of information. These are discussed in the chapter on Advanced Brain Imaging.