4 Epilepsy Syndromes
Knowing that your child has had seizures is only the beginning of the diagnostic process. The next question is: what type of epilepsy do they have? This matters because different epilepsies behave differently, respond to different treatments, and carry different long-term outlooks. Two children can both have epilepsy and yet have almost nothing else in common when it comes to their diagnosis, their care, and their prognosis.
4.1 What Is an Epilepsy Syndrome?
An epilepsy syndrome is a recognized pattern: a characteristic combination of seizure types, EEG features, age of onset, and other clinical features that tend to occur together and that carries predictable implications for treatment and prognosis.1
Epilepsy syndromes are defined and updated by the International League Against Epilepsy (ILAE), the global organization of epilepsy professionals. In 2022, the ILAE published a comprehensive formal classification of epilepsy syndromes, the most detailed and rigorous ever produced.1 Not every child with epilepsy fits neatly into a named syndrome, but when one can be identified, it significantly improves the quality of care.
4.2 How Epileptologists Think About Classification
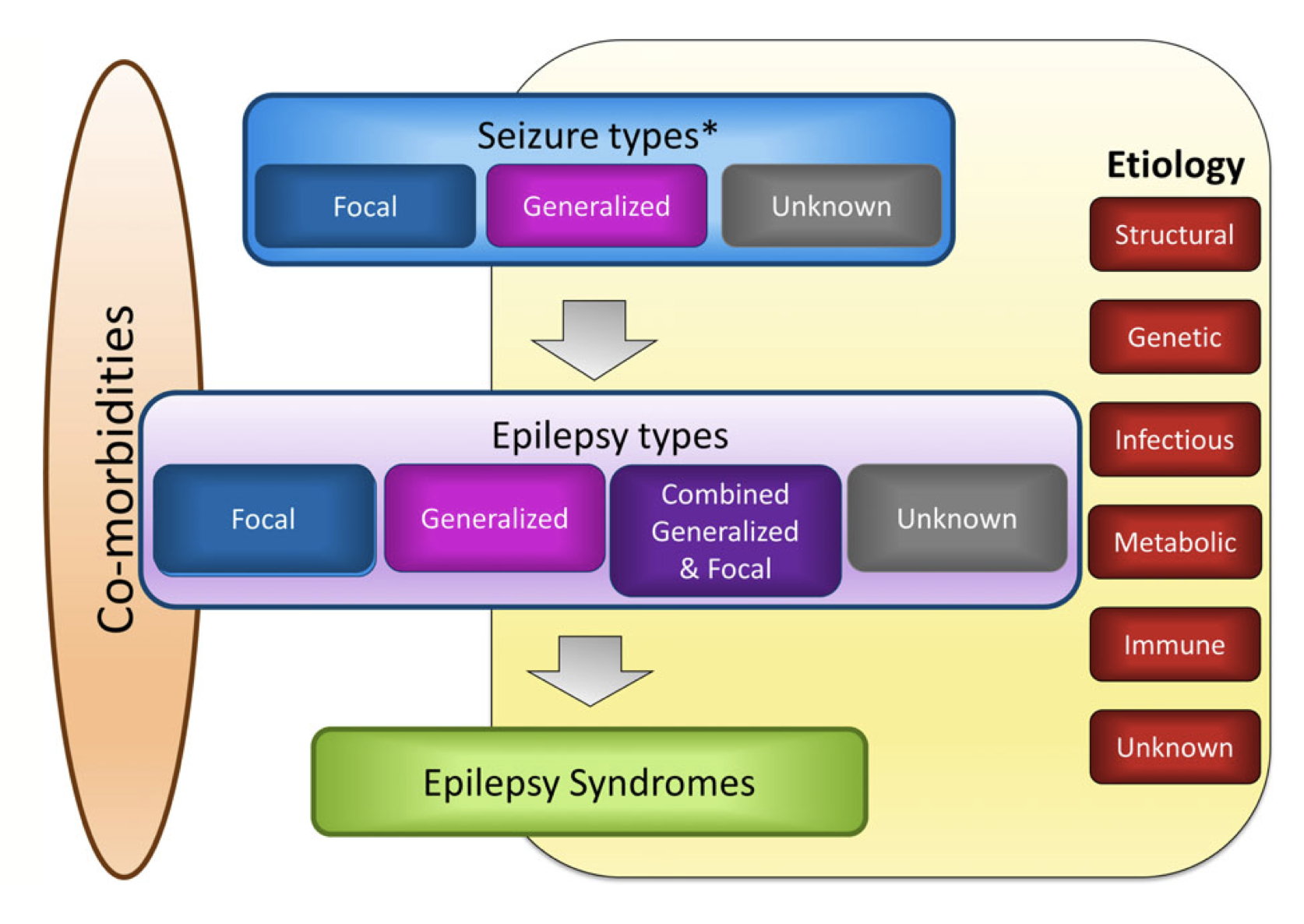
The ILAE framework organizes epilepsy across three levels that build on each other.2
The first level is the seizure type: focal, generalized, or unknown onset, as described in the previous chapter.
The second level is the type of epilepsy: focal epilepsy (seizures arising consistently from one part of the brain), generalized epilepsy (seizures involving both hemispheres from the start), combined focal and generalized epilepsy, or unknown.
The third level, when it can be determined, is the epilepsy syndrome: a specific named condition with known features, prognosis, and treatment implications.
Running alongside all three levels is the question of etiology, the underlying cause. The ILAE recognizes six broad etiological categories: structural (a visible brain abnormality), genetic (a gene variant affecting brain function), infectious, metabolic, immune, and unknown. Identifying the etiology does not replace the syndrome diagnosis; it complements it, and often helps explain why the syndrome has developed.
4.3 Why the Syndrome Diagnosis Matters
Arriving at a syndrome diagnosis, if one fits, changes care in several ways:
It may guide medication choice. Some antiseizure medications work well for certain syndromes and can actually worsen others. For example, sodium channel blockers like carbamazepine are effective for focal epilepsies but can dramatically worsen myoclonic seizures in juvenile myoclonic epilepsy or Dravet syndrome.
It shapes prognostic expectations. Childhood absence epilepsy, for instance, has an excellent prognosis, and most children outgrow it. Lennox-Gastaut syndrome, by contrast, is a lifelong condition that often requires complex, multi-modal treatment. Knowing which one a child has is essential for honest, supportive counselling.
It informs genetic counselling. Many epilepsy syndromes now have known genetic causes. A specific genetic diagnosis can explain why the epilepsy developed, predict associated features, guide targeted treatments in some cases, and allow families to make informed decisions about recurrence risk.
It determines when to consider surgery. In drug-resistant focal epilepsy, an early referral for surgical evaluation can be life-changing. In generalized epilepsy syndromes, surgery is rarely the answer, but the distinction requires a correct classification first.
4.4 Not Every Epilepsy Fits a Syndrome
It is worth saying: not every child’s epilepsy will fit neatly into a named syndrome. This is common and does not mean the diagnosis is incomplete or that something has been missed. As our understanding of epilepsy genetics deepens and new syndromes are recognized, some children who were previously unclassified will eventually receive a more specific diagnosis.